|
|
Welcome. Perhaps you've heard about safer supply from colleagues, journal articles, or other professional development activities. Or perhaps one of your patients has inquired about it. We hope this resource will answer your questions and encourage you to prescribe safer supply.
Contents
Why not just use methadone or other conventional opioid replacement therapies?
Why is safer supply a useful approach?
What evidence supports safer supply?
Don’t I need special training to prescribe safer supply?
What about infections caused by injecting tablets?
Can I consult experienced health care providers about this?
Resources to support health care providers
What is safer supply (SS)?
Because the street drug supply has become so toxic, people who rely on it are at a higher risk of harm and drug poisoning. Safer supply extends long established harm reduction models. It is a community-level approach in which physicians and nurse practitioners prescribe oral hydromorphone (Dilaudid®) tablets, often in addition to a slow-release oral morphine (Kadian® or M-Eslon®) “backbone,” to replace the toxic supply that people must otherwise rely on.
Safer supply is not for people who are new to opioids. It is a harm-reduction approach intended for adults who already rely on the toxic illegal drug supply.
Safer supply is in alignment with Health Canada’s strategy to address the drug poisoning crisis.
“I am reaching out to you, Ministers of Health, regulators of health professions and organizations representing health care practitioners, to ask you to do all you can to help provide people who use drugs with a full spectrum of options for accessing medication, depending on their individual circumstances, that will help them avoid the increased risks from the toxic drug supply. This includes your support for programs that provide greater access to a safer, pharmaceutical-grade alternative to the toxic street supply.” -- Letter from The Honourable Patty Hajdu, Minister of Health, August 24, 2020
“Naloxone access and training, supervised consumption sites and safer supply programs, are saving lives. Without these interventions in harm reduction, the number of overdose deaths would be exponentially worse.” -- Statement by The Honourable Carolyn Bennett, Minister of Mental Health and Addictions, December 15, 2021
Who supports safer supply?
Beyond Health Canada, some of the other organizations that support safer supply include:
|
|
Why not just use methadone or other conventional opioid replacement therapies?
Methadone and buprenorphine, the usual first-line treatments, work well for many people but not for everyone. A meta-analysis1 reports that mean retention in treatment after 4-6 months was 57.3% for buprenorphine and 65.5% for methadone. For some people,
- Methadone does not sufficiently suppress withdrawal symptoms
- Methadone does not fulfil their cravings
- Methadone side effects such as constipation, nausea, sleep and appetite changes, restlessness, and itchy skin can be intolerable.
People who use street drugs often face many barriers to success with traditional addictions medicine models. Such programs are often time-consuming, have rigid rules, and have limited clinic hours. In general, they are not designed with participant input or with participant needs in mind.
Why is safer supply a useful approach?
Safer supply provides additional options for people for whom methadone and other first-line drug dependency treatments have not been beneficial. The goal of methadone programs is typically eventual abstinence, while the goal for safer supply recipients is often stability, harm reduction, and increased access to health and social services.
There has been a rapid increase in fatal and non-fatal overdoses related to the illegal drug supply, and this has been exacerbated by the COVID-19 pandemic. Pandemic-related restrictions on communal spaces have led more people to use drugs alone, with no one available to respond if they overdose. Providing a safer supply of pharmaceutical grade opioids reduces risk of drug poisoning, infectious disease transmission, and death.
What evidence supports safer supply?
There is a substantial body of evidence on heroin assisted treatment (HAT) and opioid agonist treatment (OAT) built over the past 30+ years based on programs in Canada, the UK, and Europe. Safer supply providers draw on this evidence, existing clinical guidance, and best practices for harm reduction.
Evaluations from safer supply programs in Canada demonstrate positive client health outcomes and psychosocial impacts:2,3,4,5
- Improvements in health and social well-being
- Increased access to and engagement with health and social services
- Reductions in overdose and overdose risk
- Reductions in emergency department visits and hospitalizations
- Improved relationships with family members and friends
- Reductions in fentanyl use and other street-acquired drug use
- Reductions in contact with police
- Reductions in criminal activities
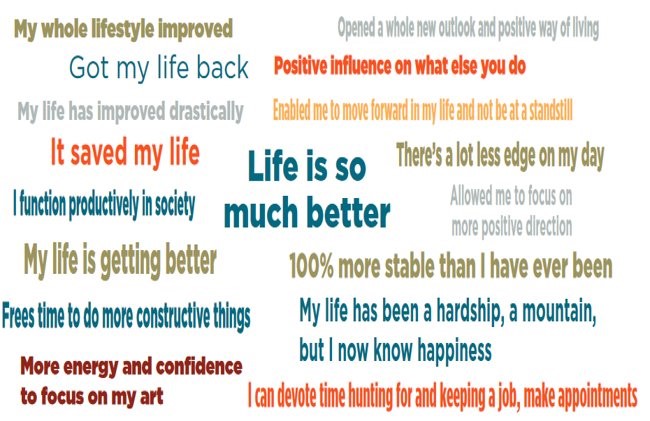
(Image: McMurchy, 2022)
See our evidence brief for more details.
What about my license?
Health care professionals are often concerned about how to stay in good standing with their regulatory college while prescribing safer supply. Experienced safer supply prescribers offer these tips:
- Keep thorough documentation of the reasoning behind your treatment decisions
- Follow clinical guidance and research evidence where it is available and appropriate
- Discuss treatment decisions, particularly any treatment decisions that may vary from clinical guidance, with experienced colleagues and document those discussions as well.
There is little publicly available information on prescriber audits and liability lawsuits, but they are not common in Canada.
Don’t I need special training to prescribe safer supply?
Health care professionals do need training — typically a single specialized course related to caring for people who have Opioid Use Disorder — before prescribing safer supply. Requirements vary across professions and across Canada, so check with your regulatory college for specifics.
Recently-graduated Nurse Practitioners (NPs) are likely to have had this training as part of their NP program.
Many regulatory colleges mention the accredited Opioid Use Disorder Treatment course run by Centre for Addiction and Mental Health (CAMH): https://www.camh.ca/en/education/continuing-education-programs-and-cour…
The Mental Health Commission of Canada has a list of opioid trainings for healthcare providers, which includes courses at CAMH and elsewhere: https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/2019-06…

What about diversion?
Diversion is the voluntary or involuntary “selling/trading, sharing or giving away of prescription medications to others”.6 The context of drug prohibition, combined with the current medical model of safer supply, has forced undue focus on the potential harms of diversion and ignored the demonstrated benefits. Breaking down the social and economic context around diversion moves us towards more shared, accurate, and compassionate understandings of diversion practices:
- Compassionate sharing: Sharing doses with partners, friends, and community members who need pain relief and/or withdrawal symptom relief.
- Survival or subsistence sharing: Sharing, exchanging, and/or selling doses to meet needs such as a place to sleep, basic physical necessities (food, water, showers, more adequate medications/ substances etc.), and/or a safe place to store doses.
- Coerced or forced diversion: Sharing, exchanging, and/or selling doses in response to threats of violence, theft, conflict, etc.
- Unintentional or inadvertent diversion: Diverting doses to others accidentally or involuntarily because of loss, violence, theft, lack of safe places to store doses, etc.
Health care provider emphasis on diversion practices can create distrust, damage patient-prescriber relationships, and result in disengagement from healthcare services.7 Health care providers and service providers build engagement when they focus on forms of health care and promotion that centre the needs, perspectives, and priorities of people who use drugs.8
For a more in-depth consideration of diversion, see the National Safer Supply Community of Practice FAQ on Reframing Diversion for Health Care Providers.
What about infections caused by injecting tablets?
Many safer supply programs prescribe Dilaudid tablets. Some program participants may choose to inject their tablets, leading to concerns about potential infections. “Infections among opioid users are indeed increasing very significantly, especially since 2016. However, infections among people with recent history of controlled-release hydromorphone have not increased. There was a small (but statistically significant) rise in infections in people with recent history of immediate-release hydromorphone, but they make up only a small percentage of people hospitalized for infections. (A majority of people with infections had a recent history of standard OAT.) These data do not support the assertion that safer supply hydromorphone is driving the increase in infection rates.” Gomes et al (2021)9
Can I consult experienced health care providers about this?
Yes. The National Safer Supply Community of Practice (NSS-CoP), a collaboration between the London InterCommunity Health Centre, the Alliance for Healthier Communities, and the Canadian Association of People who Use Drugs (CAPUD), has formal and informal prescriber mentoring available.
- Physicians and nurse practitioners can access a prescriber discussion group.
- Weekly drop-in meetings open to all NSS-CoP members (clinicians, pharmacists, program staff, people who use[d] drugs, and others). Participants discuss questions, ideas, and news.
You can join the NSS-CoP via the registration page.
Any questions? Contact info [at] nss-aps.ca (info[at]nss-aps[dot]ca) or use our Contact form.

Resources to support health care providers
A large, searchable collection of resources related to safer supply is available. A few highlights are listed below.
Clinical guidance
1. Safer Opioid Supply Programs (SOS): A Harm Reduction Informed Guiding Document for Primary Care Teams
Jessica Hales et al, 2020 (updated version coming later in 2022)
https://bit.ly/3dR3b8m
This consensus document represents the clinical experience of the authors. It aims to inform the experience and clinical knowledge of clinicians in working with people who use drugs.
2. Risk Mitigation in the Context of Dual Public Health Emergencies and Opioid Use Practice Update
BC Centre on Substance Use, 2022
https://www.bccsu.ca/covid-19/
Updated in 2022, these guidance documents were developed to provide clinical guidance around the prescribing of Safer Supply in the context of the COVID-19 pandemic. Both documents, an FAQ, several recorded webinars, and other resources are available at the above link.
3. Guidance documents from The Canadian Research Initiative in Substance Misuse (CRISM)
CRISM, 2019+
https://crism.ca/projects/covid/
CRISM produced six national rapid guidance documents addressing urgent needs of people who use substances, service providers, and decision makers in relation to the COVID‑19 pandemic. Additional resources are available for most of the guidance documents. Topics include:
- Supporting people who use substances in shelter settings during the COVID-19 pandemic
- Telemedicine support for addiction services
- Supporting people who use substances in acute care settings during the COVID-19 pandemic
- Medications and other clinical approaches to support physical distancing for people who use substances during the COVID-19 pandemic
- Strategies to reduce SARS-CoV-2 transmission in supportive recovery programs and residential addiction treatment services
- Harm reduction worker safety during the COVID-19 global pandemic
CRISM also has a national injectable opioid agonist treatment guideline. Note the many supplemental resources at the bottom of the webpage: https://crism.ca/projects/ioat-guideline/
4. Health Canada toolkit: COVID-19 and substance use
Health Canada, 2020
https://www.canada.ca/en/health-canada/services/substance-use/toolkit-s…
This toolkit was assembled to support the development of safer supply programs. It includes an FAQ about the legislative and regulatory requirements for substance use disorder treatment/safer supply, a list of all relevant exemptions that have been issued under the Controlled Drugs and Substances Act, and details of formulary coverage under drug plans of medications used for treatment and as pharmaceutical grade alternatives to the illegal supply.
5. Guide to Using Slow-Release Oral Morphine (Kadian®) in Opioid Agonist Therapy (OAT)
Équipe de soutien clinique et organisationnel en dépendance et itinérance
at the lnstitut universitaire sur les dépendances (IUD) of the CIUSSS du Centre-Sud-de-l’Île-de-Montréal, 2021
http://dependanceitinerance.ca/wp-content/uploads/2021/06/GRAPHISME-Out…
This Québec recommendation guides the use of slow-release oral morphine in cases where opioid agonist therapies with methadone or buprenorphine have been proven ineffective, unacceptable, or are contraindicated.
You can find more clinical guidance resources in the resource library.
Reports
1. Assessment of the Implementation of Safer Supply Pilot Projects
Prepared for Health Canada by Dale McMurchy Consulting, 2022
https://www.nss-aps.ca/resource/assessment-implementation-safer-supply-pilot-projects
This independent assessment report prepared by Dale McMurchy Consulting discusses impact, medications offered, services offered, program team structure, challenges, demand issues, and key features for effective safer supply program design and delivery.
2. Safer Opioid Supply Program Evaluation – Preliminary Report
London InterCommunity Health Centre, 2022
https://www.nss-aps.ca/resource/london-intercommunity-health-centres-safer-opioid-supply-program-evaluation-full-0
Clients in the safer opioid supply (SOS) program overwhelmingly appreciated the program, finding that it was reducing their overdose risk by providing a known dose of a pharmaceutical medication. They also felt that it was helping them to stabilize their health, improve their social functioning and well-being. When speaking about staff members, SOS clients referred to feeling that they are treated with respect and being provided with compassionate care that meets their health needs. LIHC staff also observed positive impacts of the SOS program on clients. However, staff also addressed the continuing negative impacts of the homelessness crisis in London on SOS clients, highlighting how this creates difficulties finding appropriate sheltering options for people living on the street and contributing to negative health and social impacts.
3. Cool Aid Community Health Centre Report on Risk Mitigation Guidance Prescriptions: Providing “Safer Supply” in CAMICO Sheltering Sites, Outreach and Primary Care Practice
Marion Selfridge et al, 2020
https://www.nss-aps.ca/resource/cool-aid-community-health-centre-report-risk-mitigation-guidance-prescriptions-providing
This report discusses a variety of outcomes, identifying populations more and less likely to continue on or benefit from safer supply prescriptions. It notes the need for a non-medical pathway to a safer drug supply.
4. Possible benefits of providing safe supply of substances to people who use drugs during public health emergencies such as the COVID-19 pandemic
Nicole Andruszkiewicz & David Gogolishvili, Ontario HIV Treatment Network, 2020
https://www.ohtn.on.ca/rapid-response-possible-benefits-of-providing-sa…
The purpose of this rapid response is to describe the benefits of providing a safe supply to people who use drugs with a focus on depressants (opioids) and stimulants. This includes examining what safe supply is, the effectiveness of various substances that can be used as safe supply, and examples where safe supply programs have been initiated in Canada (before 2020).
You can find more reports in the resource library.
Literature
1. Characterizing safer supply prescribing of immediate release hydromorphone for individuals with opioid use disorder across Ontario, Canada
Samantha Young et al, 2022
https://doi.org/10.1016/j.drugpo.2022.103601
Using provincial health data, this paper aimed to identify and characterize patients receiving safer supply immediate-release hydromorphone (IRH) and their prescribers in Ontario. Ontario. Patients prescribed safer supply IRH had demographic and clinical characteristics associated with high risk of death from opioid-related overdose. Short-term deaths among people receiving safer supply IRH were rare.
2. Injectable Opioid Agonist Treatment for Patients with Opioid Dependence: A Review of Clinical and Cost-Effectiveness
Canadian Agency for Drugs and Technologies in Health, 2020
https://cadth.ca/injectable-opioid-agonist-treatment-patients-opioid-de…
This review evaluated evidence for the clinical effectiveness and cost-effectiveness of injectable opioid agonist treatment for patients with opioid dependence. One systematic review, two randomized controlled trials, and two economic evaluations were included in the review.
3. Implementation of Safe Supply Alternatives During Intersecting COVID-19 and Overdose Health Emergencies in British Columbia, Canada, 2021
Ryan McNeil et al, 2021
https://doi.org/https://doi.org/10.2105/AJPH.2021.306692
COVID-19 disrupted British Columbia’s illegal drug market. Concerns about overdose because of drug supply changes, and deepening socioeconomic marginalization, motivated participants to access no-cost prescription alternatives. Reliable access to prescription alternatives addressed overdose vulnerability by reducing engagement with the illegal drug market while allowing greater agency over drug use. Because prescriptions were primarily intended to manage withdrawal, participants supplemented with illegal drugs to experience enjoyment and manage pain.
4. Alternatives to the toxic drug supply: an ethical analysis
Eike-Henner Kluge, 2020
Available upon request to oerc [at] gov.bc.ca (oerc[at]gov[dot]bc[dot]ca)
This paper begins with an overview of society’s duties towards its members with particular attention to the question whether it has an obligation to provide appropriate health-oriented services, relates this to the issue of addiction and the prevalence of a toxic drug supply to satisfy this addiction, and suggests an answer to some questions posed by the Ministry of Mental Health and Addictions.
5. A safer drug supply: a pragmatic and ethical response to the overdose crisis
Mark Tyndall, 2020
https://www.cmaj.ca/content/192/34/E986
Key points are that a “prohibition” approach that focuses on reducing access to pharmaceutical products directly contributes to exposure to higher risk illegal substances, which has put many people at risk of overdose; and the public health response to a poisoning epidemic must be to provide a safer alternative, which must include providing a safe supply of pharmaceutical drugs, as well as decriminalization of drug use and a redeployment of resources from enforcement to social and health services.
You can find more original research, commentaries, and literature reviews in the resource library.
Footnotes
1 Klimas, Jan, et al. “Retention in Opioid Agonist Treatment: A Rapid Review and Meta-Analysis Comparing Observational Studies and Randomized Controlled Trials.” Systematic Reviews 10, no. 1 (August 6, 2021): 216. https://doi.org/10.1186/s13643-021-01764-9. Back to text
2 Kolla, Gillian, et al. “Safer Opioid Supply Program: Preliminary Report.” London, Ontario: London InterCommunity Health Centre, November 22, 2021. https://www.nss-aps.ca/sites/default/files/resources/2022-LIHC_SOS_Program_Eval_Report.pdf. Back to text
3 McMurchy, Dale, and Robert W.H. Palmer. “Assessment of the Implementation of Safer Supply Pilot Projects.” Ottawa, Ontario, 2022. https://www.nss-aps.ca/sites/default/files/resources/2022-03-safer_supply_preliminary_assessment_report_en_0.pdf. Back to text
4 Ivsins, Andrew, et al. “‘It’s Helped Me a Lot, Just Like to Stay Alive’: A Qualitative Analysis of Outcomes of a Novel Hydromorphone Tablet Distribution Program in Vancouver, Canada.” Journal of Urban Health 98, no. 1 (February 1, 2021): 59–69. https://doi.org/10.1007/s11524-020-00489-9. Back to text
5 Selfridge, Marion, et al. “Cool Aid Community Health Centre Report on Risk Mitigation Guidance Prescriptions: Providing ‘Safer Supply’ in CAMICO Sheltering Sites, Outreach and Primary Care Practice.” Victoria, BC: Cool Aid Community Health Centre, 2020. https://coolaid.org/wp-content/uploads/2021/03/CACHC_RMG_March-August20…. Back to text
6 Larance, Briony, et al. “Definitions Related to the Use of Pharmaceutical Opioids: Extramedical Use, Diversion, Non-Adherence and Aberrant Medication-Related Behaviours.” Drug and Alcohol Review 30, no. 3 (2011): 236–45. https://doi.org/10.1111/j.1465-3362.2010.00283.x. Back to text
7 Duke, Karen, and Julie Trebilcock. “‘Keeping a Lid on It’: Exploring ‘Problematisations’ of Prescribed Medication in Prisons in the UK.” International Journal of Drug Policy 100 (February 1, 2022): 103515. https://doi.org/10.1016/j.drugpo.2021.103515. Back to text
8 Sud, Abhimanyu, et al. “Beyond Harm-Producing versus Harm-Reducing: A Qualitative Meta-Synthesis of People Who Use Drugs’ Perspectives of and Experiences with the Extramedical Use and Diversion of Buprenorphine.” Journal of Substance Abuse Treatment 135 (April 1, 2022). https://doi.org/10.1016/j.jsat.2021.108651. Back to text
9 Gomes, Tara, et al. “Trends in Hospitalizations for Serious Infections Among People With Opioid Use Disorder in Ontario, Canada.” Journal of Addiction Medicine, March 11, 2022. https://doi.org/10.1097/ADM.0000000000000928. Back to text
About this document
Adapted by the National Safer Supply Community of Practice from the Safer Opioid Supply Advocacy Tool Kit put together by staff from Street Health and Parkdale Queen West CHC.
Production of this document has been made possible through a financial contribution from Health Canada. The views expressed herein do not necessarily represent the views of Health Canada.
Version: July 2022
Suggested citation: National Safer Supply Community of Practice. (2022). Safer Supply for Health Care Providers: Frequently Asked Questions. Canada. https://www.nss-aps.ca/safer-supply-prescribers-faq
License: Creative Commons – Attribution – Noncommercial

You can share, redistribute, remix, and transform the material. (With the understanding that the citations referenced in this material are previously copyrighted by the original creators.)
You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use. Only noncommercial uses of the work are permitted.





